ISST Schroth
Basic elements of ISST training according Asklepios – Katharina Schroth
Information
Scoliosis patients need to have information about the disease to help themselves to develop pro-active coping strategies. Such information should include a calculation of the risk of progression even when it is difficult to assess accurately the risk of progression for immature children with scoliosis <25°Cobb.
To interrupt the circular process of scoliosis progression, the main therapeutic aspect is to reduce the asymmetric loading on the spine and its effects for the body statics and the postural and structural adaptations before the end of skeletal maturity.
Trained and experienced experts
PTs and physicians should have specific knowledge about radiological and clinical assessment, pathomechanism of scoliosis, documentation and scoliosis management regarding postural aspects, implementation of specific exercises, specific mobilization, and if necessary high standard braces. Because of the long term aspect of the treatment, therapists and patients must develop a special trustful relationship.
A standardized teaching process including physical examination, functional classification, documentation for therapists as well as for patients leads to an individual therapy plan followed by clearly defined follow-up evaluations.
Treatment
Specific scoliosis treatment (Asklepios Katharina Schroth), individual (out-patient by certified Schroth therapists), and possibly in groups (in-patient at the Asklepios clinic, Germany) is based on the above mentioned standardized teaching and clinical-reasoning management.
Conservative scoliosis treatment is targeting towards deceleration or prevention of progression to avoid bracing in cases with a low risk of progression and most important preventing surgery.
Treatment also includes teaching and planning scoliosis specific exercises and breathing techniques following the principles of Schroth Posture Variations to enable and encourage patients to perform a home-exercise program and achieve postural changes in activities of daily living. The intensity of the treatment program has to be individually tailored to the exercise capacity of the patients and the inherent risk of progression. Specific passive-assistive and active mobilization techniques are mandatory in case of structural-functional limitations.
Motivation, compliance, commitment, and discipline of the patients are following a deep understanding and the recognition of the main focus on long term postural changes.
Therapists should be able to accompany patients sometimes for months, years even lifelong.
Goals and main objectives
- Avoidance of surgery
- Deceleration or prevention of further progression
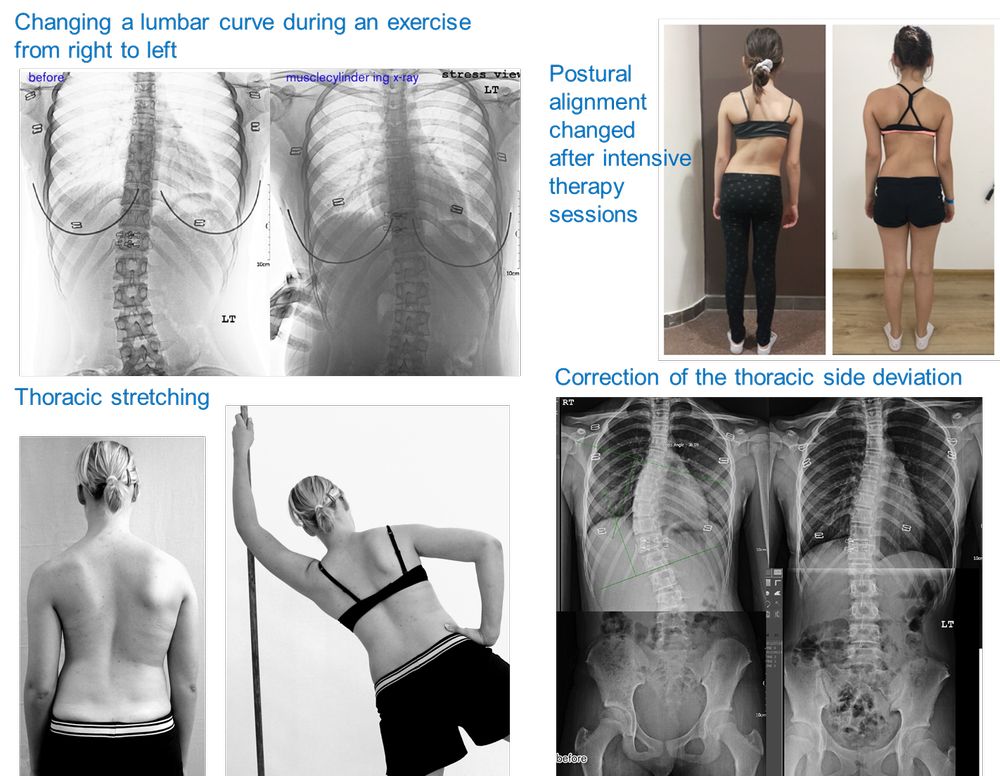
- Stabilization of spinal corrections in three dimensions
- Increase of chest mobility and respiratory function
- Trunk symmetry – cosmetic improvements
- Postural awareness and control of postural changes
- Home exercise program (HEP)
- Support regarding brace treatment – compliance – cosmetic
- Pain relief
- Help for self-help, self-competence, development of coping strategies
Standardized specific physical therapy
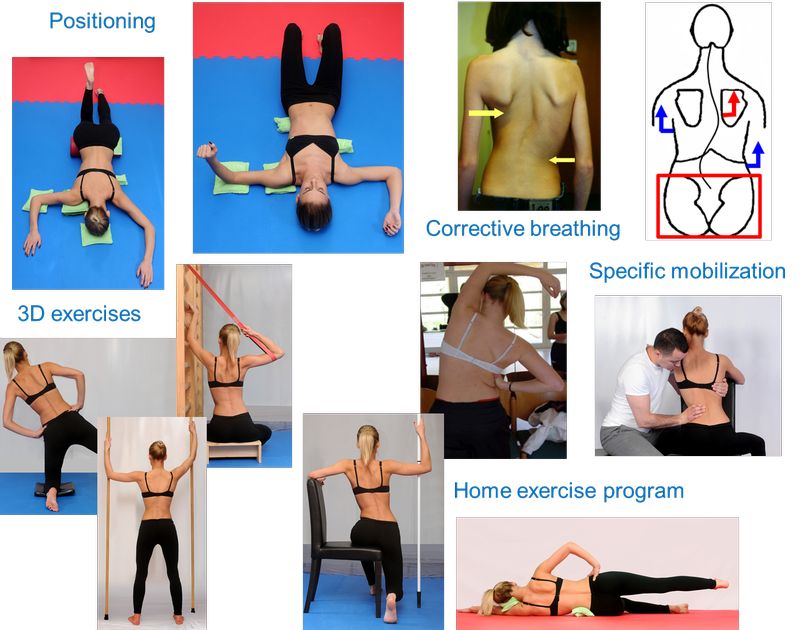
Positioning: Passive corrections for each Schroth “Body Block” up to the structural limits.
Corrective Breathing: Mobilization of the concavities by intrinsic forces.
In-brace exercises: Designed to improve the starting position for the Schroth home-exercise-program for beginners.
Specific Mobilization: Focusing on the apical segments of a curve, or soft tissues within the concavities.
3D exercises: Typical Schroth exercises try to achieve 3D corrections. Preparatory exercises could have specific goals.
Home exercise program: Essential tool to affect ADL and to prolong and intensify the correction effects
ISST – Schroth Results (1, 2, 3, 4, 5, 6)
Ref.:
1. Schreiber S, Parent EC, Moez EK, Hedden DM, Hill D, Moreau MJ, et al. The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis-an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner”. Scoliosis. 2015;10(24):1–12
2. Schreiber S. Schroth Exercises for Adolescent Idiopathic Scoliosis – Reliability, A Randomized Controlled Trial and Clinical Significance. Scoliosisjournal 2014.
3. Kuru T, Yeldan İ, Dereli EE, Özdinçler AR, Dikici F, Çolak İ. The efficacy of three-dimensional Schroth exercises in adolescent idiopathic scoliosis: a randomised controlled clinical trial. Clin Rehabil. 2016 Feb;30(2):181–90
4. Weiss HR, Weiss G, Petermann F, Incidence of progression in idiopathic scoliosis patients treated with SIR: an age and sex-matched controlled study. Pediatric Rehab., 6(1) 23-30,2003.
5. Ottmann S, Kose N. Yakut Y, The efficacy of Schroth´s 3-dimensional exercise therapy in the treatment of idiopathic scoliosis in Turkey. Saudi Med J. 26(9) 1429-1435, 2005
6. Hennes A, Goodall D, Rehabilitation (SIR) in patients with spinal deformities – Description and results. J: Physiotherapy Theory and Practice, 2009